Topographic anatomy of the legs. Topographic anatomy of the foot Topography of the human foot
The navicular tuberosity, located 3-4 cm distal to the medial malleolus, is palpable in the middle of the inner edge of the foot. The tendon of the tibialis anterior muscle is traced to the tuberosity, and outside of it is clearly visible, especially with dorsiflexion of the thumb, the tendon of m. extensor hallucis Jongus. On the outer edge of the foot, the tuberosity of the V metatarsal bone, tuberositas ossis metatarsalis V, is easily palpated. With dorsiflexion of the II-V fingers in the distal part of the foot, the tendons of m are clearly visible. extensor digitorum longus.
Dorsum border
The border of the back of the foot between the back of the foot and the sole runs outside along a line running from the middle of the height of the calcaneus to the middle of the head of the V metatarsal bone, from the inside along a line running from the middle of the height of the calcaneus to the middle of the head of the I metatarsal bone.
The skin on the back of the foot is thin and mobile. The subcutaneous tissue of the rear of the foot is loose, poor in adipose tissue. Edematous fluid easily accumulates in it. In the subcutaneous tissue of the rear of the foot, the dorsal venous arch, arcus venosus dorsalis pedis, is distally located, collecting blood from the veins of the intermetatarsal spaces. It is connected by anastomoses with the dorsal venous network of the foot, rete venosum dorsale pedis. The dorsal venous network of the foot is the source for v. saphena parva, running along the outer edge of the foot, and for v. saphena magna, which goes to the anterior surface of the medial malleolus. Nerves are located deeper than the veins: medially - branches n. saphenus, reaching the middle of the inner edge of the foot; laterally - branches n. surahs, innervating the skin of the outer edge of the foot and V toe. Most of the skin on the dorsum of the foot is innervated by the branches n. fibularis (peroneus) superficialis, the inner surface of the leafing half of the foot and I toe is the medial dorsal cutaneous nerve, n. cutaneus dorsalis medialis. The contacting surfaces of II — III, III — IV fingers are stimulated by the intermediate dorsal cutaneous nerve, item cutaneus dorsalis intermedius. The contacting sides of the IV and V fingers innervate the lateral dorsal cutaneous nerve, n. cutaneus dorsalis lateralis from n. suralis (fig.). Branches n. fibularis (peroneus) profundus innervate the skin of the contacting surfaces of I and II fingers. The fascia on the dorsum of the foot is an extension of the fascia cruris. Tendons of the long extensors and the anterior tibial muscle are connected between the leaves of its own fascia. On the sides, the fascia attaches to the I and V metatarsal bones, forming the dorsal subfascial space. The deep (inferior) wall of the space is the deep fascia that covers the metatarsal bones and the dorsal interosseous muscles. The tendons of the long extensors of the fingers and the anterior tibial muscle are surrounded by synovial sheaths, the distal border of which is at the level of the tarsometatarsal joints. The proximal border is on the anterior surface of the ankle region, just above the superior tendon retainer. In the subfascial space of the dorsum of the foot, there are short extensors of the fingers, mm. extensores hallucis brevis et digitorum brevis, as well as vessels and nerves (rice). Dorsal artery of the foot, a. dorsalis pedis, lies in the same layer with short extensors. At the level of the scaphoid (determined by its tuberosity on the inner edge of the foot), the dorsal artery of the foot lies laterally from the tendon m. extensoris hallucis longus. Here it is not covered with muscles and tendons, so you can palpate its pulsation. At the tarsal level, several small medial tarsal arteries depart from the dorsal artery of the foot to the medial side, and a rather large lateral tarsal artery to the lateral side, a. tarsalis (tarsea) lateralis. Terminal branch a. tarsalis lateralis at the lateral edge of the short extensor anastomoses with the perforating branch of the peroneal artery and participates in the formation of the lateral malleolar network, rete malleolare laterale. The distal branches anastomose with the arcuate artery at the level of the fifth metatarsal tuberosity. Arcuate artery, a. arcuata, departs from a. dorsalis pedis at the level of the tarsometatarsal joints to the lateral side. The dorsal metatarsal arteries branch off from it, aa. metatarsals (metatarseae) dorsales, and from them - the dorsal digital arteries, aa. digitales dorsales. The continuation of the main trunk of the dorsal artery of the foot is the first dorsal metatarsal artery, a. metatarsalis I, which goes to the first interdigital space. The second terminal branch of the dorsal artery of the foot is the deep plantar artery, a. (ramus) plantaris profunda, penetrates through the muscles of the first intermetatarsal space to the sole, where it anastomoses with the lateral plantar artery, a. plantaris lateralis (from a.tibialis posterior). N. fibularis (peroneus) profundus on the back of the foot is located medially from the artery. At the level of the inter-malleolar line, it gives up the motor branch to the short extensors of the fingers, which goes along with the lateral tarsal artery.
Outer outsole landmarks
On the plantar surface of the foot, you can see the longitudinal and two transverse arches. The lateral part of the longitudinal arch is formed by the calcaneus, cuboid and IV-V metatarsal bones; the medial part (spring) of the longitudinal vault consists of the talus, scaphoid, three wedge-shaped and I-III metatarsal bones. Of the ligaments in strengthening the arch of the foot, lig plays a decisive role. plantare longum - long plantar ligament. It starts from the lower surface of the calcaneus, stretches forward and is attached by deep fibers to the tuberositas ossis cuboidei and superficial - to the base of the metatarsal bones. Throwing over the sulcus ossis cuboidei, the long plantar ligament turns this groove into a bone-fibrous canal through which the tendon m. fibularis (peroneus) longus. Rice. Sole imprints (extreme right - with a flat foot). The distal transverse vault is formed by the metatarsal bones and reinforced by the transverse head m. adductor hallucis; the proximal transverse fornix is formed by the bones of the tarsus and strengthened by the tendons of m. tibialis posterior and m. fibularis (peroneus) longus. With the weakening of the strengthening apparatus, the arch descends, the foot flattens, as a result of which flat feet develop as a pathological phenomenon (Fig). Rice. Projections of the lateral and medial plantar bundles. Projection of the lateral neurovascular bundle onto the skin The projection of the lateral neurovascular bundle and intermuscular septum corresponds to the line from the middle of the sole width (or from the middle of the line connecting the tops of the ankles) to the fourth interdigital space. The medial bundle is projected along a line drawn from the middle of the inner half of the sole width to the first interdigital space (Fig.).
The skin of the sole is inactive, thickened, especially on the calcaneal tuberosity, the heads of the metatarsal bones and along the lateral edge of the foot. It is firmly connected by connective tissue septa with the plantar aponeurosis. The innervation of the skin is shown in Fig. The subcutaneous tissue of the sole is dense and has a cellular structure. This layer is especially developed above the calcaneus and above the metatarsophalangeal joints: its thickness here reaches 1.0-1.5 cm. There is no superficial fascia of the plantar surface of the foot. Plantar aponeurosis. Fascial beds of the sole. Plantar aponeurosis, aponeurosis plantaris, in the middle of the sole is a thickened fascia of its own. On the sides of it, the fascia becomes thinner and attaches to the bones of the tarsus, and distally - to the I and V metatarsal bones. The plantar aponeurosis has a particularly dense structure in the tarsal region, where part of the flexor flexor fibers of the fingers begins from it. In the metatarsal region, the aponeurosis splits into 4-5 legs that cover the flexor tendons of the fingers. As in the palm of the hand, in the distal region, these legs are interconnected by transverse bundles, fasciculi transversi, limiting the commissural openings. The commissural openings are filled with fatty tissue, the tendons of the worm-like muscles are located here and the common digital vessels and nerves exit, aa. et nn. digitales plantares communes. Through the commissural openings of the plantar aponeurosis, the subcutaneous tissue communicates with the middle fascial bed of the sole. The medial and lateral fascial intermuscular septa extending from the edges of the plantar aponeurosis divide the subaponeurotic space of the sole into three fasial beds: medial (muscle bed of the first finger), middle and lateral (muscle bed of the fifth finger). The medial intermuscular septum is attached to the calcaneus, scaphoid, medial sphenoid and I metatarsal bones, the lateral - to the long ligament of the sole and to the V metatarsal bone (Fig.). Middle fascial bed of the sole The lower wall of the middle fascial bed is formed by the plantar aponeurosis. The upper wall of the middle fascial bed in the tarsal region is formed by the long ligament of the sole and the bones of the tarsus, in the metatarsal region - by the deep fascia that covers the plantar interosseous muscles. The lateral walls of the middle fascial bed are the medial and lateral intermuscular septa.
Borders: the lower limb (extremitas inferior) is bounded in front by the sulcus inguinalis, lateral-crista iliaca, behind by the line connecting the spina iliaca posterior superior with the coccyx, medial-perineal-femoral fold. Division into areas: gluteal (regio glutea), thigh (femur), lower leg (crus), foot (pes).
The gluteal region. Borders : upper - crista iliaca, lower - sulcus glutealis, lateral - the line connecting the upper anterior spine with the greater trochanter, medial - os sacrum, os coccygis. External landmarks : iliac crest, anterior and posterior superior iliac spine, ischial tubercle, greater trochanter of the femur, sacrum and coccyx, gluteal fold, intergluteal fold.
Hip. Borders: upper - inguinal ligament and inguinal fold, lower - a line drawn 2 transverse fingers above the patella, lateral - a line connecting the anterior edge of the greater trochanter with the lateral epicondyle of the thigh, medial - a vertical line from the pubic symphysis to the medial epicondyle of the thigh. External landmarks: anterior superior iliac spine, pubic tubercle and crest, anterior edge of the greater trochanter, medial femoral condyle, patella; anterior thigh muscle group, adductors, inguinal ligament.
Knee. Borders: upper - transverse line, located 4 cm above the upper edge of the patella, lower - at the level of tuberositas tibiae. Two vertical lines drawn along the posterior edges of the femoral condyles separate the regio genu anterior from the regio genu posterior. External landmarks: patella, biceps and semi-membranous muscles, heads of the gastrocnemius muscle, transverse skin fold, head of the fibula, medial edge of the tibia and condyle of the femur.
Shin. Borders: the upper one is a line drawn through the tuberositas tibiae, the lower one is a line drawn through the bases of the ankles. External landmarks: the front edge of the tibia, the head of the fibula.
Foot. The border feet - a horizontal line drawn through the base of the ankles. Regio dorsalis pedis and regio plantaris pedis are distinguished on the foot. External landmarks: malleolus lateralis et medialis, tuber calcaneus, I and V metatarsal bones.
The gluteal region. Layers their characteristics : 1.Skin (cutis). 2.Subcutaneous adipose tissue (panniculus adiposus). Clunium superiors, medii et inferiores branch out in it. Musculo-fascial beds: 3.lamina superficialis fasciae gluteae covers the gluteus maximus muscle. 4. Superficial layer of muscles: m. gluteus maximus 5. lamina profunda fasciae gluteae separates the gluteus maximus muscle from the deep fat layer. 6.stratum adiposum 7.Middle layer of muscles: m. gluteus medius; m. piriformis; m. gemellus superior et inferior - tendo m. obturatorii interni; m. quadratus femoris. 8. Deep layer of muscles: m. gluteus minimus; m. obturatorius externus. 9. Bone base of the pelvis: facies posterior sacri, ossa coxae. Cellular spaces : the subgluteal space is communicated: through the supra- and sub-piriform opening with the lateral cellular tissue space of the pelvis; through the small sciatic foramen from the ischial - rectal fossa; through the gap under the proximal part of the gluteus maximus tendon with the lateral and anterior regions of the thigh; along the sciatic nerve - with fiber of the posterior fascial bed of the thigh.
Hip ... Layers anterior thigh and their characteristics: 1.Cutis, 2.Panniculus adiposus, 3.Fascia superficialis, 4.Fascia lata gives 3 intermuscular septa: external, internal and posterior, which divide the subfascial space of the thigh into muscle-fascial beds: anterior, containing the extensor muscles of the leg, posterior, containing flexor muscles, medial, containing the adductor muscles of the thigh 5. The superficial layer of the muscles of the anterior region of the thigh forms 2 triangles - medial and lateral. Trigonum femorale mediale is limited from the inside by m.gracilis, from the outside by m.sartorius, from above by lig.inguinale. Trigonum femorale laterale is bounded from the inside by m.sartorius, from the outside by m.tensor fasciae latae, from below by a horizontal line bordering the regio genus. In the medial, 3 muscles lie: outside — m.iliopsoas, medial — m.pectineus, even more medial — m.adductor longus. The tissue of the medial fascial bed of the femur communicates through the obturator opening with the prevesical or lateral cellular tissue space of the small pelvis. In the lateral, 3 heads of m.quadriceps femoris are superficially overlain. 6. Deep layer of muscles: in trigonum femorale mediale-m.adductor brevis and even deeper-m.adductor minimus; in trigonum femorale laterale-m.vastus intermedius and m.articularis genus.
Back thigh layers and their characteristics: 1. Derma, 2. Panniculus adiposus, 3. Fascia superficialis, 4. Fascia lata 5. Superficial layer of muscles: m.biceps femoris, m.semitendinosus, m.semimembranosus. Thigh muscles: anterior group: m. quadriceps femoris consists of m.rectus femoris, m.vastus medialis, m.vastus lateralis et m.vastus intermedius, m. sartorius. Back group: m.semimembranosus, m. semitendinosus, m. biceps femoris, composed of caput longum and caput breve. Medial group: m.pectineus, m. adductor brevis, m. adductor longus, m. adductor major, m. gracilis. The femoral triangle (trigonum femorale) is bounded from above by lig.inguinale, outside m. sartorius, inside m. adductor longus. It contains a, v, n femoralis.
Cellular spaces: the fiber located along the sciatic nerve communicates with the following spaces: above with the fiber space under the gluteus maximus muscle, below with the popliteal fossa fiber, through the hiatus adductorius and the adductor canal with the fiber spaces of the anteromedial thigh.
Knee. Layers of the anterior knee area and their characteristics: 1.Cutis, 2.Panniculus adiposus. 3.Fascia superficialis between the leaves contains bursa subcutanea praepatellaris and bursa subcutanea infrapatellaris located in front of the tuberosity
tibia. 4.Fascia propria is a continuation of the fascia lata of the thigh, from below it passes into the fascia cruris. The bursa subfascialis prepatellaris can be located under the fascia propria. 5. Tendo m. quadricipitis femoris is thrown over the patella and becomes lig. patellae. In the same layer, retinaculum patellae mediale et retinaculum patellae laterale are located on the sides of the patella. Bursa subtendinea praepatellaris can be located between the tendon of the quadriceps muscle and the patella. 6. The patella is the largest sesamoid bone of the human skeleton. Above the patella, under the tendon of the quadriceps muscle-bursa suprapatellaris, which communicates with the joint cavity, under the patellar ligament is the bursa infrapatellaris profunda, containing the corpus adiposus infrapatellare.
Layers of the back of the knee and their characteristics: 1.Cutis, 2.Panniculus adiposus. 3.Fascia superficialis. 4.Fascia poplitea is a continuation of the wide fascia of the thigh, from top to bottom passes into the fascia cruris. 5.Fossa poplitea. Medially and from above, the popliteal fossa is limited by m. semimembranosus et m. semitendinosus, laterally and from above - m. biceps femoris, from below laterally and medially - respectively caput laterale et caput mediate m. gastrocnemii. 6. Facies poplitea femoris, posterior surface of the knee joint capsule with lig. popliteum obliqum and m. popliteus form the bottom of the popliteal fossa.
Cellular spaces: the fatty tissue of the popliteal fossa is reported: at the top - along the sciatic nerve with the fiber of the sparing part of the thigh; through the hiatus adductorius along the popliteal vessels - with the fiber of the anterior region of the thigh; downward through the hole bounded by the tendon arch m.soleus - with the fiber of the posterior deep space of the leg.
Shin. Shin layers and their characteristics: 1.Cutis, 2.Panniculus adiposus 3.Fascia superficialis. 4.Fascia cruris - continuation of the fascia lata of the thigh, below it passes into the fascia dorsalis pedis. The fascia of the lower leg gives off septum intermusculare anterior et septum intermusculare posterior. On the front surface of the lower leg, 2 Musculo-fascial beds: anterior and lateral. Compartimentum cruris anterius is bounded in front by its own fascia, posteriorly by the interosseous membrane, medial-tibial bone, lateral-anterior intermuscular septum of the tibia. Compartimentum cruris laterale in front is limited by the anterior intermuscular septum, laterally - by its own fascia, medially - by the fibula and behind - by the posterior intermuscular septum. In the anterior fascial bed, m lies medially. tibialis anterior, outwards from it - m. extensor digitorum longus, and between them, starting from the middle third, - m. extensor hallucis longus, the neurovascular bundle of the anterior fascial bed of the lower leg includes a.tibialis anterior, vv.tibiales anterior, n. peroneus profundus. In the lateral bed are mm. fibulares longus et brevis. The superficial part of the posterior fascial bed is occupied by 2 heads of the gastrocnemius muscle and m. soleus, m. plantaris, deep - m. flexor digitorum longus, m. flexor hallucis longus, m.tibialis posterior. Cellular spaces: deep tissue of the lower leg lies along the neurovascular bundle and communicates upward with the tissue of the popliteal fossa, downward - along the deep flexor tendons, through canalis malleolaris with the cellular tissue of the sole.
Foot. Layers of the back of the foot and their characteristics: 1.Cutis; 2.Panniculus adiposus; 3.fascia superficialis; 4.fascia propria, splitting into 2 leaves, forms a bed for the tendons of the m.tibialis anterior and long extensors. 5. Deep fascia - covers the dorsal interosseous muscles. 6.Muscles of the back of the foot: first layer: m. extensor hallucis longus; m. extensor digitorum longus; the second is m.extensor digitorum brevis; m. extensor hallucis brevis; third- m. interosseus dorsalis pedis.
Layers of the sole of the foot and their characteristics: 1.Cutis; 2.Panniculus adiposus; 3.fascia superficialis is fused with the plantar aponeurosis; 4.fascia propria - thickening, forms a plantar aponeurosis. From the plantar aponeurosis, 2 partitions go deeply, which, together with the interosseous septum, limit 4
Musculo-fascial beds: deep bed - filled with interosseous muscles; middle bed - contains m.flexor digitorum brevis (lies superficially),
and deeper - m.quadratus plantae, tendons m.lumbricales, m.flexor digitorum longus, m.adductor hallucis; the medial bed - contains the muscles of the thumb: mm.flexor hallucis brevis, abductor hallucis and tendon m.flexor hallucis longus; laterally - contains the muscles of the little finger: mm.abductor et flexor digiti minimi breves.
5.Muscles of the big toe: m. abductor hallucis, m. flexor hallucis brevis. 6. Middle muscle group: the first layer of muscles - m. flexor digitorum brevis; second layer: m. quadratius plantae, tendo m. flexoris digitorum longi, mm. lumbricales; third layer: m. adductor hallucis, tendo m. peronaei longi; fourth layer: mm. interossei plantares, mm. interossei dorsales. Muscles of the little finger: m. abductor digiti minimi, m. flexor digiti minimi brevis, m. opponens digiti minimi.
The space under the inguinal ligament is divided into muscle and vascular lacunae... The lacunae of the thigh are separated by the ilio-comb arch.
Muscle lacuna(lacuna musculorum) bounded in front by the inguinal ligament, medially by the arcus iliopectineus, behind and laterally by the ilium. Through the muscle lacuna on the thigh pass m. iliopsoas, n. femoralis and n. cutaneus femoris lateralis.
Vascular lacuna(lacuna vasorum) bounded in front by lig.inguinale, behind - lig.pectineale, medially - lig. lacunare, laterally - arcus iliopectineus. Femoralis and v pass through the vascular lacuna. femoralis, lymph node.
Suprapiriform opening (foramen suprapiriformis) between the ischial notch and the superior edge of the piriformis muscle. The internal opening of the canal faces the subperitoneal space of the pelvic cavity. The outer opening of the canal faces the deep cellular space of the gluteal region. A., V pass through the hole. et n. gluteus superior.
Piriform opening (foramen infrapiriforme) in the lower part of the greater sciatic foramen, located between the lower edge of the piriformis muscle and the sacrospinous ligament. A., V pass through the under-ear-shaped opening. et n. gluteus inferior, n. ischiadicus, and a. pudenda interna et v. pudenda interna et n. pudendus and n.cutaneus femoris posterior.
Femoral canal(canalis femoralis) is formed when a hernia passes through the femoral ring. The walls of the femoral canal: anterior - upper horn of the crescent edge, posterior - fascia pectinea, lateral - v.femoralis. The inner ring of the femoral canal is limited: in front - lig.inguinale, behind - lig.pectineum, medially - lig.lacunare, laterally - v.femoralis. The outer ring of the femoral canal is formed by margo falciformis fasciae latae. The content of the femoral canal is a femoral hernia.
Leading channel(canalis adductorius). Walls: anterior-lateral - m.vastus medialis, posterior-medial - m. adductor magnus, front - lamina vastoadductoria, thrown between these muscles and covered by m. sartorius.
Through the upper opening, a canal enters the channel. et v. femoralis, n. saphenus; through the front exit a. genus descendens, n. saphenus; through the lower, located between the tendon m. adductor magnus and femur, a, vv.femoralis extend into the popliteal fossa. The adduction canal connects the anterior fascial bed of the thigh with the popliteal fossa.
Locking channel(canalis obturatorius) is located in the obturator hole. It contains a., V. et n.obturatoriae. Limited from above by sulcus obturatorius ossis pubis, from below - membrana obturatoria, m. obturatorius int. et m. obturatorius ext.
Calf-popliteal canal(canalis cruropopliteus). The anterior wall is the posterior tibial muscle, the long flexor of the fingers. Back wall - deep
a leaf of the fascia of the leg, the soleus muscle adjacent to it. The upper opening of the channel is limited in front of m. popliteus, behind-arcus tendineus m. solei. Through the upper opening, a canal enters the channel. et v. poplitea and n. tibialis. The anterior opening is located on the interosseous membrane. Through it, the anterior tibial artery and vein penetrate into the anterior muscle bed. The lower opening is a slit-like passage from under the medial edge of the gastrocnemius muscle. The posterior tibial artery and veins pass through it and n comes out. tibialis.
Superior peroneal canal(canalis musculoperonaeus superior) - between the fibula and the long peroneal muscle. It contains n. peroneus communis, which is divided by n. peroneus superficialis et profundus.
Inferior peroneal canal(canalis musculoperonaeus inferior) bounded laterally by the fibula, behind by the long flexor of the big toe, in front by m.tibialis posterior. The channel hosts a.et v.tibiales posterior.
Medial ankle canal(canalis malleolaris medialis) consists of 4 fibrous containers: a tendo m.tibialis passes through the first canal behind the ankle
posterior; through the second - tendo m. flexoris digitorum longi; through the third pass a. et v. tibialis posteriors and n. tibialis; through the fourth canal-tendo m. flexor hallucis longus.
Lateral ankle canal (canalis malleolaris lateralis) - serves as a receptacle for tendo mm. peronaei longus et brevis.
Ankle dorsal canals(canalis talocruralis). The tendo m.tibialis anterior passes through the medial; through the middle - m.extensor hallucis longus, a.et v.tibialis anterior, n.peronaeus profundus; through the lateral 4 tendons of m.extensor hallucis longus.
Calcaneal canal- the gap between the calcaneus and the abductor thumb muscle. A dense aponeurotic septum divides it into 2 sections: posterior and anterior. In the back is m.quadratus plantae, the external plantar neurovascular bundle passing in the splitting of the fascia. In the anterior are the tendons of the long flexor of the thumb and the long flexor of the fingers, in the septum separating the square muscle from the tendons, the medial neurovascular plantar bundle passes.
Plantar canal(canalis plantaris) is located in the proximal part of the deep fascial space of the middle bed of the sole. Borders: upper lig.plantare longum, lower-deep fascia covering the long flexor of the fingers with a square muscle, lateral-wall of the outer bed and m. quadratus plantae, medial wall of the inner bed. In canal, loose tissue, square muscle and plantar, lateral and medial vascular bundles.
The gluteal region. 1.The superior gluteal neurovascular bundle emerges from the epigastric foramen: a.glutea superior supplies blood to the piriformis muscle, gluteus maximus, middle and small muscles. The veins of the same name, forming a plexus, cover the superior gluteal artery, and n.gluteus superior, is located downward and outward in relation to the vessels and innervates the listed muscles.
2. Through the under-pear-shaped opening exit: - n. ischiadicus, from which n.cutaneus femoris posterior, a.comitans n.ischiadici go medially. The sciatic nerve is directed from top to bottom of it, the superior twin muscle, the tendon of the internal obturator muscle, the lower twin and square muscles.
- a.glutea inferior is surrounded by the veins and branches of the same name n.gluteus inferior. In the opening, the bundle lies medially from the sciatic nerve and the posterior cutaneous nerve of the thigh. Coming out of the hole, the artery and nerve break up into branches that penetrate into the thickness of the gluteus maximus muscle and into the piriformis muscle.
- the genital neurovascular bundle (a. Et v. Pudendae internae and n. Pudendus) is located in the piriform opening most medially. Coming out of the hole, the bundle lies on the sacrospinous ligament and the spine of the ischium, then passes through the small sciatic foramen under the sacroiliac ligament to the inner surface of the ischial tuberosity. The exit site of the upper nerves of the buttock in the area of the Pirogov spine, the middle cutaneous nerves - on the line of the beginning of the gluteus maximus muscle between the posterior and superior iliac spine and the base of the coccyx, the lower cutaneous nerves - along the lower edge of the gluteal muscle, respectively, in the middle of the gluteal fold. The projection of the superior gluteal artery in the position of rotation of the thigh inward is determined slightly below the middle of the line connecting the spina iliaca posterior superior with the lateral edge of the ischial tuberosity. At the same point, the projection of the lower gluteal nerve, the posterior cutaneous nerve of the thigh and the sciatic nerve is determined.
Hip. Neurovascular bundles: projection onto the skin surface, syntopy of their elements: aa take part in the blood supply to the thigh. femoralis et obturatoria. The femoral artery is a continuation of the external iliac artery. Ken's projection: line from mid-distance between the anterior superior iliac spine and symphysis to the tuberculum adductorium on the medial femoral condyle. After leaving the vascular lacuna, the artery enters the femoral triangle, located between the vein lying medially and the nerve that goes to the thigh through the muscle lacuna (VAN).
Obturator neurovascular bundle: the vessels and nerve leave the obturator canal on the thigh. The obturator artery departs from the anterior branch of the internal iliac artery or from a.epigastrica inf, passes through the obturator canal into the medial group of the thigh muscles. After leaving the canal, it is divided into r.anterior, which supplies the muscles of the medial group, anastomosed with the medial artery, which envelopes the femur,
r.posterior, blood supply to the proximal parts of the muscles of the posterior group, r. acetabularis, giving rise to the artery of the ligament of the femoral head.
Venous outflow: v. saphena magna flows into v. femoralis. V. saphena magna is projected along the line: the lower point is the posterior edge of the medial femoral condyle, the upper point is at the border of the medial and middle third of the inguinal ligament.
Knee. Neurovascular bundles: projection onto the skin surface, syntopy of their elements: superficial nerves and vessels of the anterior region of the knee pass: 1) n.saphenus and ramus cutaneus n. obturatorii, innervating the skin of the medial regions of the region. 2) rr. cutanei anteriores n. femoralis, innervating the skin of the central parts of the region. 3) n. cutaneus femoris lateralis-innervates the skin of the lateral regions of the region. 4) rete patellaris, formed by a. genus descendens, aa.
genus superiores medialis et lateralis, aa. genus inferiores medialis et lateralis, a. recurrens tibialis anterior. The rete articulare genus is located under its own fascia, supplying blood to the anterior parts of the knee joint and the surrounding tissues. The neurovascular bundle of the popliteal fossa. Its projection is a vertical line drawn through the middle of the popliteal fossa. As part of the neurovascular bundle-a. et v. poplitea, n. tibialis. An artery is located in front and medially, a vein is located lateral and behind it, a nerve is even more lateral and behind (i.e., the mnemonic code NeVA).
A. poplitea enters the popliteal fossa from the lower opening of the adducting canal, then enters the upper opening of the canalis cruropopliteus. Projection line a. poplitea: the top point of the line is on the border of the inner and middle third of the upper knee diameter, the bottom point is in the middle of the lower knee diameter. In the neurovascular bundle, the artery has an anteromedial position.
V. poplitea lies in the popliteal fossa laterally and behind the artery of the same name, through the lower opening into the canalis adductorius, where v. femoralis. N. tibialis at the level of the joint space is projected in the middle of the popliteal region, located in the popliteal fossa lateral and behind the popliteal vein, branches to the posterior muscle group of the lower leg and n. cutaneus surae medialis. N. peroneus communis passes at the lateral border of the popliteal fossa, its projection is the medial edge of the biceps femoris. Under the muscles limiting the popliteal fossa are located: bursa anserina, bursa subtendinea m. gastrocnemii medialis and bursa m. semimembranosi.
Shin. Neurovascular bundles: projection onto the skin surface, syntopy of their elements: projection of the neurovascular bundle of the anterior region of the leg: a.tibialis anterior- line from the middle of the distance between the head of the fibula and the tuberosity of the tibia to the middle of the distance between the inner and outer ankles. N.fibularis superficialis - along the line from the posterior edge of the fibular head to the anterior edge of the lateral malleolus. V.saphena magna and n.subcutaneus - along a line running from the posterior edge of the medial condyle of the femur to the anterior edge of the medial malleolus. Projection of the neurovascular bundle of the posterior region of the leg: a.tibialis posterior - along the line from the middle of the transverse skin fold of the popliteal fossa to the middle of the distance between the posterior edge of the medial malleolus and the medial edge of the Achilles tendon. A. fibularis - along a line drawn from a point lying medially from the head of the fibular bone to the posterior edge of the lateral malleolus. V.saphena parva and n. cutaneus surae medialis in the upper half of the area - along a line running in the middle of the back surface.
A.tibialis anterior departs from a. poplitea passes through the opening in the interosseous membrane and lies on its anterior surface medial to the deep peroneal nerve, descends with it, passing along the outer edge of the anterior
tibial muscle. Its branches: a. recurrens tibialis anterior, involved in the formation of rete patellaris; a. malleolaris anterior lateralis forming rete malleolare laterale; a. malleolaris anterior medialis, going to the area of the inner ankle, where it forms rete malleolare mediale. The anterior tibial artery is accompanied by vv. tibiales anteriores, flowing into the ankle-popliteal canal in v. poplitea. A.tibialis posterior, accompanied by 2 veins of the same name and n.tibialis, leaves the ankle-popliteal canal through the lower opening. Coming out of it, the neurovascular bundle is directed to the 3 channel behind the medial malleolus. Branches branch off from the posterior tibial artery: a. circumflexa fibulae participates in the formation of the rete articularis genus; rami malleolaris medialis participate in the formation of rete malleolare mediale; rami calcanei mediates take part in the formation of rete calcaneum. peronea crosses the posterior tibial muscle and penetrates into canalis musculoperoneus inferior in the middle third of the lower leg. Its branches: r.perforans forms rete malleolaris lateralis and rete calcaneum; a. malleolaris lateralis forms rete malleolaris lateralis; rami calcanei laterales form rete calcaneum A. tibialis posterior accompanied by vv. tibiales posteriores, the accompanying peroneal artery vv flow into them. pegonae. After the fusion of the posterior tibial veins with vv. tibiales anteriores formed by v. poplitea.
Foot. Neurovascular bundles: projection onto the skin surface, syntopy of their elements: Rear of the foot: this is a.v.dorsales pedis and n.peroneus profundus. The artery goes between the tendons mm.extensor digitorum longus et extensor hallucis longus, and before reaching the 1st interdigital space, gives a.arcuata (which passes under the m.extensor hallucis brevis and gives a.metatarseae dorsales, from which aa.digitales are formed dorsales, a.metatarseae dorsalis prima and ramus plantaris profundus, which goes to the foot through the first intermetatarsal space and participates in the formation of arcus plantaris.Nerve - goes inwardly from the artery and gives branches to the adjacent sides of the 1st and 2nd fingers.Innervates the short extensor digitorum.
Projection of blood vessels and nerves on the foot: branches n. peroneus superficialis- lines running from a point above the lateral ankle at a distance of 10-12 cm from its apex. A. Dorsalis pedis and n. peroneus profundus - a line going from a point lying in the middle of the ankle line to the I interdigital space. A. plantaris laterali - a line running from the posterior edge of the medial malleolus to the outer edge of the base of the V finger. A. plantaris medialis-line running from the posterior edge of the medial malleolus to the I interdigital space.
The sole of the foot: Medial neurovascular bundle (a.v.n. plantares mediales) - go to the sulcus plantaris medialis.
Lateral neurovascular bundle (a.v.n. plantares laterales) - goes to the sulcus plantaris lateralis At the level of the base of the metatarsal bones, the artery passes into the arcus plantae. The arch anastomoses with the deep plantar branch of the a.dorsalis pedis. From them aa.metatarseae plantares depart, from which aa.digitales plantares are formed. The plantar region is innervated by n. plantaris medialis et lateralis.
Collateral circulation in occlusion of the femoral artery: when dressing in the upper third of the thigh above the place of origin of the deep artery of the thigh, blood circulation can be carried out: 1) from a. glutea inferior through anastomosis with r. ascendens a. circumflexae femoris lateralis, 2) from a. obturatoria through anastomosis with an ascending branch a. circumflexa femoris medialis. When ligating an artery in the middle and lower third of the thigh, the roundabout blood circulation is due to the descending branches of the medial and lateral arteries that go around the femur.
Collateral circulation in popliteal artery occlusion: when ligating a.poplitea between the upper and lower arteries of the knee joint, collateral circulation is carried out through two collateral arcs: between aa. genus superior and inferior (minor arc) and between a. genus descendens and a. recurrens tibialis anterior (large arch). When dressing in the distal section, i.e. below the place of origin aa. genus inferiores to the site of division of the popliteal artery into the anterior and posterior tibial arteries, collateral arches are located above the ligature. Below it, the anastomosis remains, and the recurrencies of the tibialis anterior, due to which, in the main, the connection with the vessels of the lower leg is carried out.
Collateral circulation with occlusion of the tibial artery: with occlusion of the anterior tibial artery, collateral circulation is carried out due to the popliteal and posterior tibial arteries and their branches, and with occlusion of the posterior tibial artery - due to the popliteal and anterior tibial arteries and their branches.
Zones of sensory and motor innervation of N. femoralis- runs outward from the femoral artery. Within the femoral triangle below the inguinal ligament, the femoral nerve is divided into terminal branches: 1) the rami musculares innervate the quadriceps femoris muscle and the sartorius muscle. 2) rami cutanei anteriores innervate the skin of the front of the thigh. 3) n. saphenus - innervates the skin of the anteromedial surface of the leg and foot. N. genitofemoralis - its r. femoralis innervates the skin of the upper medial thigh and the muscle that lifts the testicle.
Zones of sensory and motor innervation of N. obturatorius- leaves the pelvis through the obturator canal, gives off rami musculares that innervate the medial muscle group of the thigh, ramus cutaneus, which innervates the lower part of the medial surface of the thigh, and sensitive branches to the hip joint.
Zones of sensory and motor innervation of N. ischiadicus- comes out of the pelvis through the foramen infrapiriforme, lies along the midline in the groove between caput longum m. biceps femoris from the posterolateral side, mm. semitendinosus et semimembranosus from the posteromedial side and m. adductor magnus in front. On the thigh, the sciatic nerve innervates the semitendinosus, semimembranosus and long head of the biceps femoris.
Zones of sensory and motor innervation of N. peronaeus supetficialis. The nerve descends in the upper muscular-peroneal canal to the level of the middle of the lower leg, pierces the fascia of the lower leg and enters the mass of fatty deposits. It innervates the lateral muscle group of the lower leg and the skin of the lateral surface of the lower leg and dorsum of the foot.
Zones of sensory and motor innervation of N. peronaeus profundus. The nerve bends around the neck of the fibula, pierces the anterior intermuscular septum and lies on the interosseous membrane in the upper third of the lower leg between the anterior tibial muscle and the extensor longus of the fingers lateral to the anterior tibial artery. It innervates the anterior leg muscles and the skin of the first interdigital space on the foot. n. tibialis innervates all muscles of the posterior group.
Hip joint(articulatio coxae) formed by acetabulum and caput ossis femoris. Along the edge of the acetabulum, the fibrous-cartilaginous acetabular lip is attached, spreading over the incisura acetabuli in the form of a lig. transversum acetabuli. The lunar surface surrounds the fossa acetabuli. The lig begins from the fossa of the head. capitis femoris, heading to the acetabular notch, where it attaches to the lig. transversum acetabuli. In the ligament of the femoral head, there is an artery that supplies the femoral head - r. acetabularis a. obturatoriae. Capsula articularis is attached along the edge of the acetabulum with the location of the acetabular lip in the joint cavity, and on the os femoris it is fixed along the linea intertrochanterica in front and back-inward from crista intertrochanterica between the outer and middle third of the femoral neck. The hip joint is covered in front by the pubic-femoral ligament, ilio-comb fascia, rectus femoris muscle, iliopsoas muscle. Bundles: lig. iliofemoorale extends from the lower anterior iliac spine to the intertrochanteric line; lig. ischiofemorale extends from the posterior edge of the acetabulum and ischial tuberosity to the greater trochanter and the lateral part of the intertrochanteric crest; lig. pubofemorale extends from the superior ramus of the pubic bone to the inferior part of the intertrochanteric line.
Features of the structure of the hip joint in children: the hip joint in newborns has a thin stretched capsule. The posterior superior part of the joint capsule is not reinforced with ligaments, and the edge of the acetabulum is smoothed. In the first year of life, the ilio-femoral ligament is lengthened, which increases the angle of extension in the hip joint. With further growth, the ischio-femoral ligament is formed. The blood supply to the femoral head is mainly due to the artery of the femoral head ligament. After synostosis of the femoral head and neck (at the age of 15-16), anastomoses are formed between the branches supplying the femoral neck and the branches of the artery of the femoral head ligament, therefore, the value of the latter in the blood supply to the femoral head decreases.
Knee-joint(articulatio genus) form the distal epiphysis of the femur, the proximal epiphysis of the tibia and the patella. The distal end of the femur expands downward and forms the condylus medialis et condylus lateralis, for articulation with the articular surfaces of the tibia. The articular capsule consists of fibrous and synovial membranes1) membrana fibrosa, it is strengthened by ligaments: lig. patellae and retinaculum patellae mediate et retinaculum patellae laterale, lig. collaterale fibulare, lig. popliteum obliquum, lig. popliteum arcuatum, lig. transversum genus). 2) membrane synovialis forms intra-articular folds: plica synovialis infrapatellaris, plicae alares, bursa infrapatellaris profunda. Intracapsular ligaments: lig. cruciatum anterius, lig. cruciatum posterius, lig. meniscofemorale posterius. Synovial bags: bursa suprapatellaris, bursa anserina, bursa subtendinea m. gastrocnemii medialis,
bursa subtendinea m. gastrocnemii lateralis. The innervation of the joint comes from n.peroneus - outside, n.femoralis - from the inside and n.tibialis - from behind. The blood supply to the knee joint is from the rete articularis genus. Lymphatic drainage from the anterior part of the knee joint occurs in the inguinal lymph nodes, from the posterior to the popliteal.
Features of the structure of the knee joint in children: the joint of the newborn has a rounded shape, the contours of the patella and its ligaments are hardly noticeable. The epiphyses of the femur and tibia, which form the knee joint, are formed by cartilaginous tissue containing the nuclei of ossification; the patella is entirely formed by cartilage tissue. The outer condyle of the thigh is more developed than the inner one. By the age of two, the size of the condyles is leveled. The patellar ligament itself strengthens the joint bag in front. The oblique and arcuate popliteal ligaments are poorly expressed. The cruciate ligaments are dense and short.
Ankle joint
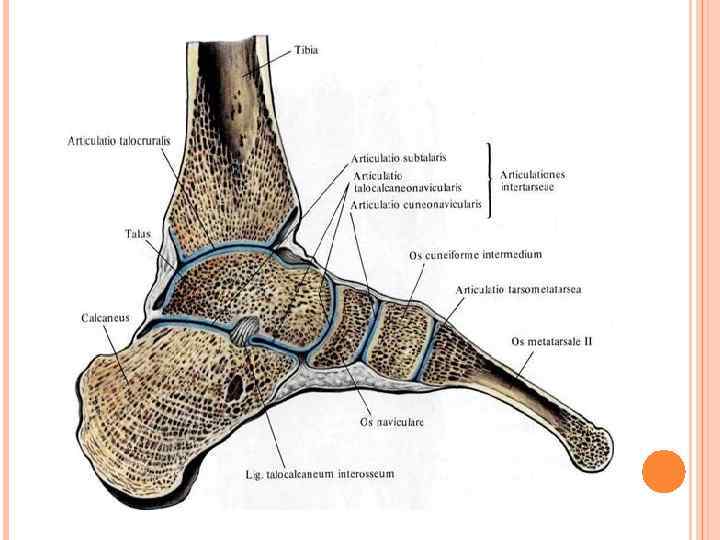
(articulatio talocruralis) is formed by the distal epiphyses of the lower leg bones and the talus, which are connected by the anterior and posterior tibiofibular ligaments. The joint is block-shaped in shape. The articular capsule is attached along the edge of the articular cartilage, reinforced with ligaments from the sides. The lig departs from the medial ankle. mediale. Three ligaments extend from the lateral ankle: lig. talofibulare anterius, lig. talofibulare posterius, lig. calcaneofibulare. The blood supply to the anterior part of the articular capsule is carried out by a. tibialis anterior, posterior - a. tibialis posterior, and external due to a.peronea. N takes part in the innervation of the joint capsule. saphenus, n. suralis, and n. peroneus profundus.
Features of the structure of the joint in children: in newborns, the joint is formed by the cartilaginous epiphyses of the lower leg bones and the cartilaginous talus. The ankle capsule is very thin, the ligaments are poorly developed, especially the deltoid.
The gluteal region. the lymphatic vessels of the region end in the inguinal nodes (superficial) and in the nodes of the pelvic cavity (deep).
Hip. Lymphatic vessels and regional lymph nodes: the lymphatic system of the thigh is represented by vasa lymphaticum superficiale et profundum, as well as nodi lymphatici inguinales profundi and superficial inguinal lymph nodes, among the latter, nodi lymphatici inguinales superficiales superolaterales, superomediales et inferiores are distinguished. Superficial lymphatic vessels collect lymph from superficial tissues, flow into nodi lymphaiici inguinales superficiales inferiores. Deep inguinal lymphatic vessels collect lymph from deep
sections of the limb, follow along the medial surface of the femoral vein, flow into the deep inguinal lymph nodes, then into nodi limphatici iliaci externi.
Knee. Lymphatic vessels and regional lymph nodes: lymphatic drainage from the anterior part of the knee joint occurs in nodi lymphatici inguinales superficialis inferiors, from the posterior - in nodi lymphatici popliteales, from the latter, lymph flows into the lower superficial inguinal lymph nodes. Nodi lymphatici poplitealis profundi among 5-6 are located in the popliteal fossa near
popliteal vessels.
Shin. Lymphatic vessels and regional lymph nodes: superficial lymphatic vessels flow into nodi lymphatici inguinales and nodi lymphatici popliteales. In the course of the anterior tibial arteries and veins, deep lymphatic vessels pass, flowing into nodi lymphatici tibiales anteriores, located in the upper third of the leg; the outflowing vessels from these nodes flow into nodi lymphatici popliteales.
Foot. Lymphatic vessels and regional lymph nodes. Llymph from the back of the foot flows into nodi lymphatici inguinales superfaciales inf. Lymphatic drainage of the plantar surface of the foot through the vessels accompanying vv. saphena magna et parva. The lymphatic vessels of the medial edge of the foot go along the great saphenous vein of the leg to the inner surface of the lower leg and thigh to the inguinal lymph nodes. Vessels of the outer edge of the foot accompany the small saphenous vein of the leg and flow into the popliteal lymph nodes.
Surgical anatomy of congenital malformations:
1. Clubfoot - congenital contracture of the joints of the foot. The foot is in the flexion position at the ankle joint, its outer edge is lowered, and the anterior section is adducted and bent with an increase in the longitudinal arch. Ligaments and bursae on the medial side of the foot atrophy. The posterior tibial muscle and the long flexor of the thumb are shortened, and their tendons are thickened. The calcaneal tendon is also thickened. The peroneal muscles are usually hypotrophic, their tendons are mixed posteriorly.
2. Hip dislocation - the ratios of the hip joint are disturbed: the head of the femur is located outside the acetabulum, first at its level, with age, sliding along the wing of the iliac bone, it gradually shifts up and back. The articular bag takes the shape of an hourglass, which creates obstacles in repositioning the dislocation. The gluteal muscles are relaxed due to the displacement of the femoral head, and their atrophy gradually sets in. A child with bilateral congenital dislocation of the hip walks, waddling from foot to foot, limping in case of unilateral dislocation.
The plantar canal is located on the tarsus in the proximal part of the deep fascial space of the middle bed of the sole (I.D.Kirpatovsky). It is formed from above (from the rear) lig. Plantare longum, and below (from the sole) by a deep fascia covering the long flexor of the fingers with a square muscle. Laterally, it borders on the wall of the outer bed and the outer leg of m. Quadratus plantae (tarsal fascial cell fissure), medially with the wall of the inner bed. Proximally, the plantar canal passes into the calcaneal, and distally - into the anterior part of the deep fascial space of the middle bed of the sole, between the tendons of the long flexor of the fingers and the adductor muscle of the big toe.
The plantar canal contains loose tissue, the square muscle, closely associated with the long flexor tendon of the fingers, and the plantar, lateral and medial, vascular bundles.
On the metatarsal plantar canal passes into a narrow gap between the tendons of m. Flexor digitorum longus and m. Adductor hallucis. The gap is filled with fiber; on the sides it is closed by the cases of the flexors of the thumb and V fingers. A., vv. Et n. Plantares mediales emerge from under the abductor thumb muscle, at a distance of 7 to 8 cm from the calcaneal tuberosity. The bundle passes at the junction of the deep fascia of the middle bed with the wall of the inner bed and is slightly covered by the edge of m. Abductor hallucis.
At the level of the transition of the abductor muscle of the thumb into the tendon, the superficial branch a. Plantaris medialis and branch n. Plantaris medialis extends medially from the flexor hallucis longus tendon. Deep branches run between the heads of the flexor hallucis short, covering the tendon m. Flexor hallucis longus. Throughout the entire length of division into branches, the nerve most often runs along the outer edge of the artery. At the exit from the commissural openings, the arterial branches intersect with nerve branches.
A., vv. Et n. Plantares laterales extend from under the edge of the abductor thumb muscle at a distance of 4 - 5 cm from the calcaneal tuberosity. The vessels and nerve run arcuate from the inside to the outside and from back to front to the inner-posterior edge of the abductor muscle of the V finger. First, the bundle passes in the splitting of the deep fascia of the middle bed, and then (in the metatarsal region) at the junction between the deep fascia and the outer bed of the sole. The lateral plantar nerve extends medially from the artery. N. Plantaris lateralis at the level of the base of the V metatarsal bone (the artery is somewhat distal) is divided into superficial and deep branches.
The superficial branches enter the subcutaneous tissue through the fourth commissural opening and the outer edge of the middle part of the plantar aponeurosis, heading to the IV-V fingers. The superficial arterial branch goes to the outer surface of the V finger.
The deep branches of the artery and nerve are directed into the interval between the oblique head of the adductor thumb muscle, the fourth dorsal and third plantar interosseous muscles. The artery forms a deep plantar arch on the interosseous muscles, and the nerve gives branches to the interosseous muscles.
At the bases of the intermetatarsal spaces, the plantar arterial arch anastomoses with the branch of the medial plantar artery, and with the posterior perforating branches with a. Arcuata (from a. Dorsalis pedis). More often in the 1m intermetatarsal space arcus plantaris and a. Arcuata are connected via r. Plantaris profundus (from a. Dorsalis pedis). At the heads of the metatarsal bones under the transverse head m. Adductor hallucis, the metatarsal arteries pass into the common digital arteries. All arterial branches are accompanied by veins of the same name.
"Surgical anatomy of the lower extremities", V.V. Kovanov
Leather dense, inactive.
Subcutaneous tissue dense, lobed, reaches the greatest thickness at the points of support. Permeated with dense connective tissue bundles connecting the skin with the underlying aponeurosis of the sole.
Own fasz Iya of the sole in the middle section is represented by the plantar aponeurosis (aponeurosis plantaris), which extends from the calcaneal tuberosity to the heads of the metatarsal bones. Aponeurosis consists of longitudinal and transverse tendon fibers. At the level of the heads of the metatarsal bones, the transverse and longitudinal fibers of the aponeurosis form commissural foramen. Internal and external fascial intermuscular septa depart from the edges of the plantar aponeurosis. The internal intermuscular septum is attached to the calcaneus, scaphoid, medial sphenoid and I metatarsal bones; the outer is fixed to the V metatarsal bone. They divide the entire space under the plantar aponeurosis into three sections: the medial - or the muscle bed of the first finger, lateral - or the muscle bed of the fifth finger and the median.
In the medial bed the following muscles lie: muscle, abductor I finger (m. abductor hallucis), short flexor of I finger (m. flexor hallucis brevis) and tendons of the long flexor of the first finger (m. flexor hallucis longus).
The lateral muscle group is represented by the abductor little finger muscle (m. abductor digiti minimi), little finger flexor muscle (m. flexor digiti minimi), muscle opposing the V finger (m. opponens digiti minimi).
In the median fascial bed, immediately below the aponeurosis, are located: flexor digitorum short (m. flexor digitorum brevis), square muscle of the sole (m. quadratus plantae) and flexor digitorum longus tendon (m. flexor digitorum longus) with worm-like muscles starting from them (mm. lumbricales)... The oblique and transverse heads of the muscle leading the I finger are located deeper (m. adductor hallucis),, obliquely crosses the sole of the peroneus longus tendon.
The plantar interosseous muscles are enclosed by the interosseous fascia in a separate bed.
The blood supply and innervation of the plantar surface of the foot is carried out by the medial and lateral plantar vessels and nerves.
There are 2 grooves between the muscle beds: slow (sulcus plantaris medialis)(located between the short flexor of the fingers and the muscles of the first finger) and lateral (sulcus plantaris lateralis)(located between the short flexor of the fingers and the muscles of the little finger). The vessels and nerves of the sole pass through them.
In the ankle canal, the posterior tibial artery and the tibial nerve are divided into branches: the medial and lateral plantar vessels and nerves that pass to the sole into the calcaneal canal (located between the calcaneus and the muscle that abducts the first finger). Having passed through the calcaneal canal, the vessels enter the medial and lateral plantar grooves.
Medial plantar vessels and nerve (a. plantaris medialis et n. plantaris medialis) are sent to the medial plantar sulcus.
Lateral plantar vessels and nerve (a. plantaris lateralis et n. plantaris lateralis) at first they are located in the median bed between the flexor short of the fingers and the square muscle of the sole, then they pass into the lateral plantar groove. At the level of the heads of the metatarsal bones, the lateral plantar artery passes again into the median bed, where, by anastomosing with the deep plantar branch from the dorsal artery of the foot, it participates in the formation of the plantar arch (arcus plantaris). The plantar metatarsal arteries extend from the plantar arch (aa. metatarseae plantares), which give rise to the common plantar digital arteries (aa. digitales plantares communes), the latter are divided into their own plantar digital arteries (aa. digitales plantares propriae)(the finger's own artery extends to the outer edge of the little finger directly from the lateral plantar artery).
Projection
Medial plantar neurovascular bundle is projected along a line drawn from the middle of the inner half of the sole width to the first interdigital space.
Lateral plantar neurovascular bundle is projected along a line drawn from the middle of the width of the sole (or from the middle of the line connecting the tops of the medial and lateral malleolus) to the 4th interdigital space.
Cellular spaces
In the middle fascial bed, the following cellular spaces are distinguished.
Subgaleneurotic cellular cleft - between the plantar aponeurosis and the flexor digitorum short. It is closed proximally, distally passes into the VFA of the sole through the commissural foramen.
Superficial cellular cleft - between the flexor digitorum short and the tendons of the long finger flexor. It is connected proximally with the plantar and calcaneal canals, distally - with interdigital tissue.
A deep cellular gap is between the tendons of the long flexor of the fingers and the muscle that adducts the first finger. Associated with the fiber of the plantar canal and interdigital spaces.
The medial and lateral fascial beds do not contain a large accumulation of tissue and do not have pronounced cellular gaps.
Ways of spreading purulent streaks from the middle fascial bed
On the dorsum of the foot along the deep plantar branch of the dorsal artery of the foot and along the vermiform muscles.
Into the VFA of the sole through the commissural foramen of the plantar aponeurosis.
In the posterior fascial bed of the lower leg. The middle bed communicates with the deep lower leg bed through three channels. The plantar canal is connected to the middle bed, which passes proximally into the heel canal; the latter passes into the ankle, communicating with the deep bed of the posterior region of the lower leg.
In the medial bed of the sole along the tendon of the muscle adducting the 1st finger.
In the lateral bed of the sole along the tendon of the 5th toe from the long flexor of the toes.
 The lower limb consists of a pelvic girdle and a free lower limb. The border runs from the pubic tubercle, along the inguinal fold, the anterior superior iliac spine, the iliac crest to the base of the sacrum.
The lower limb consists of a pelvic girdle and a free lower limb. The border runs from the pubic tubercle, along the inguinal fold, the anterior superior iliac spine, the iliac crest to the base of the sacrum.
 Free lower limb Pelvic girdle Glute area Anterior thigh area Rear thigh area Anterior knee area Rear knee area Anterior lower leg area Rear lower leg area Ankle ankle Rear ankle area of the foot (rear and sole) Toe area
Free lower limb Pelvic girdle Glute area Anterior thigh area Rear thigh area Anterior knee area Rear knee area Anterior lower leg area Rear lower leg area Ankle ankle Rear ankle area of the foot (rear and sole) Toe area
 Gluteal region Borders: upper - along the iliac crest, lower - along the gluteal fold, medial - along the median line of the sacrum and coccyx, lateral - the line connecting the anterior superior iliac spine with the greater trochanter of the femur.
Gluteal region Borders: upper - along the iliac crest, lower - along the gluteal fold, medial - along the median line of the sacrum and coccyx, lateral - the line connecting the anterior superior iliac spine with the greater trochanter of the femur.
 LAYER-LAYER TOPOGRAPHY OF THE Gluteal REGION Skin of the PZhK Fascia: - Superficial - Own: - lumbar - iliac - gluteus muscles: - Superficial layer - gluteus maximus muscle - Middle layer - gluteus maximus, pyriform, internal obturator, upper, lower twin muscles, square muscles. - Deep layer - gluteus minimus, external obturator
LAYER-LAYER TOPOGRAPHY OF THE Gluteal REGION Skin of the PZhK Fascia: - Superficial - Own: - lumbar - iliac - gluteus muscles: - Superficial layer - gluteus maximus muscle - Middle layer - gluteus maximus, pyriform, internal obturator, upper, lower twin muscles, square muscles. - Deep layer - gluteus minimus, external obturator
 BLOOD SUPPLY AND INERVATION OF THE Gluteal REGION In the supra-piriform foramen, the upper SNP (superior gluteal artery, vein, nerve) passes through the sub-pyriform foramen. hips. Lymph flows into the groin l / y. The sciatic nerve projects at a point midway between the sciatic tuberosity and the greater trochanter (most superficial location).
BLOOD SUPPLY AND INERVATION OF THE Gluteal REGION In the supra-piriform foramen, the upper SNP (superior gluteal artery, vein, nerve) passes through the sub-pyriform foramen. hips. Lymph flows into the groin l / y. The sciatic nerve projects at a point midway between the sciatic tuberosity and the greater trochanter (most superficial location).
 PELVIC JOINT A simple joint is formed by the acetabulum of the pelvic bone and the head of the femur. The articular surface of the pelvic bone is enlarged by the fibrocartilaginous acetabular lip, fused with the edge of the acetabulum.
PELVIC JOINT A simple joint is formed by the acetabulum of the pelvic bone and the head of the femur. The articular surface of the pelvic bone is enlarged by the fibrocartilaginous acetabular lip, fused with the edge of the acetabulum.

 MOVEMENT IN THE HIP JOINT 1) 2) 3) Around the frontal axis - flexion at 84 -1200, extension at 130; Around the sagittal axis - adduction and abduction of the lower limb in relation to the midline 80 - 900; Around the vertical axis - rotation of the femoral head in general by 40 -500.
MOVEMENT IN THE HIP JOINT 1) 2) 3) Around the frontal axis - flexion at 84 -1200, extension at 130; Around the sagittal axis - adduction and abduction of the lower limb in relation to the midline 80 - 900; Around the vertical axis - rotation of the femoral head in general by 40 -500.
 BOUNDARIES OF THE ANTERIOR REGION OF THE THIGH Upper - inguinal ligament Lower - transverse line running 2 transverse fingers above the patella Lateral - lines connecting the middle of the pubic symphysis with the medial condyle of the thigh and the greater trochanter with the lateral condyle of the thigh.
BOUNDARIES OF THE ANTERIOR REGION OF THE THIGH Upper - inguinal ligament Lower - transverse line running 2 transverse fingers above the patella Lateral - lines connecting the middle of the pubic symphysis with the medial condyle of the thigh and the greater trochanter with the lateral condyle of the thigh.
 LAYER-LAYER TOPOGRAPHY OF THE ANTERIOR THIGH REGION Skin of the pancreas Fascia: - superficial (superficial and deep sheets) - own (wide) (deep and superficial plates) Muscles: - anterior group (quadriceps femoris muscle, sartorius muscle) - posterior group (thin, comb and 3 leading - long, short and large muscles).
LAYER-LAYER TOPOGRAPHY OF THE ANTERIOR THIGH REGION Skin of the pancreas Fascia: - superficial (superficial and deep sheets) - own (wide) (deep and superficial plates) Muscles: - anterior group (quadriceps femoris muscle, sartorius muscle) - posterior group (thin, comb and 3 leading - long, short and large muscles).
 BOUNDARIES OF THE HINDER THIGH REGION Upper - gluteal fold Lower - continuation of a circular line drawn two transverse fingers above the patella Lateral - lines connecting the middle of the pubic symphysis with the medial femoral condyle and the greater trochanter with the lateral femoral condyle.
BOUNDARIES OF THE HINDER THIGH REGION Upper - gluteal fold Lower - continuation of a circular line drawn two transverse fingers above the patella Lateral - lines connecting the middle of the pubic symphysis with the medial femoral condyle and the greater trochanter with the lateral femoral condyle.
 LAYERAL TOPOGRAPHY OF THE HINDHIP REGION PZhK Skin Fascia Broad Fascia Muscles - extensors of the thigh and flexors of the lower leg (biceps femoris, semitendinosus muscle, semimembranosus muscles)
LAYERAL TOPOGRAPHY OF THE HINDHIP REGION PZhK Skin Fascia Broad Fascia Muscles - extensors of the thigh and flexors of the lower leg (biceps femoris, semitendinosus muscle, semimembranosus muscles)
 BLOOD SUPPLY AND INERVATION OF THE HIP The SNP is a deep artery, a vein of the thigh and the sciatic nerve. Venous and lymphatic drainage is directed upward and laterally, into the femoral vein and inguinal l / y. The skin is innervated by the posterior and lateral cutaneous nerves, and the muscles are innervated by the sciatic nerve.
BLOOD SUPPLY AND INERVATION OF THE HIP The SNP is a deep artery, a vein of the thigh and the sciatic nerve. Venous and lymphatic drainage is directed upward and laterally, into the femoral vein and inguinal l / y. The skin is innervated by the posterior and lateral cutaneous nerves, and the muscles are innervated by the sciatic nerve.
 KNEE. BORDERS. Upper - a circular line drawn two transverse fingers above the patella Lower - a circular line drawn two transverse fingers below the patella Vertical lines drawn through the epicondyle of the thigh divide the line into anterior and posterior.
KNEE. BORDERS. Upper - a circular line drawn two transverse fingers above the patella Lower - a circular line drawn two transverse fingers below the patella Vertical lines drawn through the epicondyle of the thigh divide the line into anterior and posterior.
 LAYER-LAYER TOPOGRAPHY OF THE ANTERIOR KNEE REGION PZhK skin Fascia - superficial - own (continuation of fascia lata)
LAYER-LAYER TOPOGRAPHY OF THE ANTERIOR KNEE REGION PZhK skin Fascia - superficial - own (continuation of fascia lata)
 KNEE JOINT Complex, formed by the articular surfaces of the condyles of the femur, tibia and the posterior articular platform of the patella. The joint is strengthened by ligaments: - intra-articular cruciate (anterior, posterior) extra-articular: collateral - peroneal and tibial, oblique and arcuate popliteal and patellar ligament proper.
KNEE JOINT Complex, formed by the articular surfaces of the condyles of the femur, tibia and the posterior articular platform of the patella. The joint is strengthened by ligaments: - intra-articular cruciate (anterior, posterior) extra-articular: collateral - peroneal and tibial, oblique and arcuate popliteal and patellar ligament proper.
 KNEE JOINT The joint is blocky-rotational in shape. Axes of rotation: - frontal - flexion-extension with an amplitude of 140 -1600 - vertical
KNEE JOINT The joint is blocky-rotational in shape. Axes of rotation: - frontal - flexion-extension with an amplitude of 140 -1600 - vertical
 BOUNDARIES OF THE POPLEGE FOSS Upper outside - biceps of the thigh Internal - semitendinosus and semimembranosus muscles Lower - medial and lateral heads of the gastrocnemius muscle
BOUNDARIES OF THE POPLEGE FOSS Upper outside - biceps of the thigh Internal - semitendinosus and semimembranosus muscles Lower - medial and lateral heads of the gastrocnemius muscle
 LAYER-LAYER TOPOGRAPHY OF THE PEGLENAL FOUNTAINS Skin of the PZhK Fascia - superficial - own (superficial and deep leaves)
LAYER-LAYER TOPOGRAPHY OF THE PEGLENAL FOUNTAINS Skin of the PZhK Fascia - superficial - own (superficial and deep leaves)
 BLOOD SUPPLY AND INERVATION OF THE POPLITEAL FOOM SNP - popliteal artery and vein, tibial nerve. In the upper corner of the fossa, the sciatic nerve is divided into the tibial and common peroneal nerves. The femoral artery, leaving the adduction canal, lies in the popliteal fossa, where its continuation is called the popliteal artery. The popliteal vein is formed from the confluence of the four tibial veins, anterior and posterior.
BLOOD SUPPLY AND INERVATION OF THE POPLITEAL FOOM SNP - popliteal artery and vein, tibial nerve. In the upper corner of the fossa, the sciatic nerve is divided into the tibial and common peroneal nerves. The femoral artery, leaving the adduction canal, lies in the popliteal fossa, where its continuation is called the popliteal artery. The popliteal vein is formed from the confluence of the four tibial veins, anterior and posterior.
 SHIN. BORDERS. Upper - a transverse line drawn through the tibial tuberosity; Lower - a transverse line passing through the base of the ankles; Vertical lines drawn through the ankles and epicondyle of the thigh divide the area into anterior and posterior areas.
SHIN. BORDERS. Upper - a transverse line drawn through the tibial tuberosity; Lower - a transverse line passing through the base of the ankles; Vertical lines drawn through the ankles and epicondyle of the thigh divide the area into anterior and posterior areas.
 LAYERAL TOPOGRAPHY OF THE ANTERIOR REGION OF THE SHIN Skin of the pancreas Fascia - superficial - own Muscles - anterior group - extensors of the leg and foot (anterior tibial muscle, extensor longus of the fingers, long extensor of the thumb) - lateral group - peroneal muscles (long, peronealis muscle) ...
LAYERAL TOPOGRAPHY OF THE ANTERIOR REGION OF THE SHIN Skin of the pancreas Fascia - superficial - own Muscles - anterior group - extensors of the leg and foot (anterior tibial muscle, extensor longus of the fingers, long extensor of the thumb) - lateral group - peroneal muscles (long, peronealis muscle) ...
 BLOOD SUPPLY AND INERVATION OF THE ANTERIOR REGION OF THE SHIN The anterior tibial artery and deep peroneal nerve are projected along a line drawn from the middle of the distance between the tuberosity of the tibia and the peroneal head from above to the middle of the distance between the ankles below. The saphenous vein of the leg and the saphenus are projected along the line connecting the medial malleolus and medial epicondyle of the thigh. Lymphatic drainage from the bottom up and laterally into the popliteal l / u.
BLOOD SUPPLY AND INERVATION OF THE ANTERIOR REGION OF THE SHIN The anterior tibial artery and deep peroneal nerve are projected along a line drawn from the middle of the distance between the tuberosity of the tibia and the peroneal head from above to the middle of the distance between the ankles below. The saphenous vein of the leg and the saphenus are projected along the line connecting the medial malleolus and medial epicondyle of the thigh. Lymphatic drainage from the bottom up and laterally into the popliteal l / u.
 LAYER-LAYER TOPOGRAPHY OF THE BACK REGION OF THE TIBS Skin of the pancreas Fascia - superficial - own (superficial and deep) Muscles - superficial (triceps, plantar muscles) - deep long flexor of the fingers, pancake flexor of the thumb, posterior tibial muscles).
LAYER-LAYER TOPOGRAPHY OF THE BACK REGION OF THE TIBS Skin of the pancreas Fascia - superficial - own (superficial and deep) Muscles - superficial (triceps, plantar muscles) - deep long flexor of the fingers, pancake flexor of the thumb, posterior tibial muscles).
 BLOOD SUPPLY AND INVERVATION OF THE POSTERIUM REGION OF THE SHIN The tibial nerve, together with the posterior tibial veins and the artery, is projected along a line connecting a point located one transverse toe posteriorly from the medial edge of the tibia to the middle of the distance between the inner ankle and the Achilles tendon. The saphenous vein is projected in the groove between the heads of the gastrocnemius muscle.
BLOOD SUPPLY AND INVERVATION OF THE POSTERIUM REGION OF THE SHIN The tibial nerve, together with the posterior tibial veins and the artery, is projected along a line connecting a point located one transverse toe posteriorly from the medial edge of the tibia to the middle of the distance between the inner ankle and the Achilles tendon. The saphenous vein is projected in the groove between the heads of the gastrocnemius muscle.
 LAYERAL TOPOGRAPHY OF THE ANTERIOR AND HINDER ANKLE Anterior region Posterior region Skin of the subcutaneous tissue Own fascia - superior ligament (transverse) - inferior ligament (cruciate) Skin of the subcutaneous tissue Fascia own Between the calcaneal tuberosity and the tendon there is a bursa
LAYERAL TOPOGRAPHY OF THE ANTERIOR AND HINDER ANKLE Anterior region Posterior region Skin of the subcutaneous tissue Own fascia - superior ligament (transverse) - inferior ligament (cruciate) Skin of the subcutaneous tissue Fascia own Between the calcaneal tuberosity and the tendon there is a bursa
 BLOOD SUPPLY AND INERVATION OF THE ANTERIOR AND HINDER AREAS OF THE ANTERIOR JOINT The blood supply is carried out by the anterior tibial artery and its continuation - the dorsal artery of the foot. Venous outflow in the proximal direction to the popliteal vein. Lymphatic drainage - into the popliteal lymph nodes. Innervation is carried out by the saphenous nerve and the superficial peroneal nerve, muscles - by the deep peroneal nerve.
BLOOD SUPPLY AND INERVATION OF THE ANTERIOR AND HINDER AREAS OF THE ANTERIOR JOINT The blood supply is carried out by the anterior tibial artery and its continuation - the dorsal artery of the foot. Venous outflow in the proximal direction to the popliteal vein. Lymphatic drainage - into the popliteal lymph nodes. Innervation is carried out by the saphenous nerve and the superficial peroneal nerve, muscles - by the deep peroneal nerve.
 LATERAL TOPOGRAPHY OF THE LATERAL AND MEDIAL ANKLE Lateral region Medial region Skin of the peroneal muscles The intrinsic fascia forms two ligaments of the tendon retainer of the peroneal muscles Skin of the peroneal muscles Fascia forms the retainer of the flexor tendon
LATERAL TOPOGRAPHY OF THE LATERAL AND MEDIAL ANKLE Lateral region Medial region Skin of the peroneal muscles The intrinsic fascia forms two ligaments of the tendon retainer of the peroneal muscles Skin of the peroneal muscles Fascia forms the retainer of the flexor tendon
 ANKLE JOINT The joint is complex, formed by the block and ankle surfaces of the talus, articular surfaces of the ankles and the lower articular surface of the tibia. The composition is block-shaped. Movement: dorsal extension and plantar flexion. Ligaments strengthen the joint from all sides: medial and three lateral.
ANKLE JOINT The joint is complex, formed by the block and ankle surfaces of the talus, articular surfaces of the ankles and the lower articular surface of the tibia. The composition is block-shaped. Movement: dorsal extension and plantar flexion. Ligaments strengthen the joint from all sides: medial and three lateral.
 BORDERS OF THE FOOT Upper - the line connecting the tops of the ankles, drawn through the back and sole of the foot. On the sides, lines drawn from the middle of the calcaneus to the head of the I metatarsal bone inside and to the tuberosity of the V metatarsal bone outside divide the area into the back and the sole.
BORDERS OF THE FOOT Upper - the line connecting the tops of the ankles, drawn through the back and sole of the foot. On the sides, lines drawn from the middle of the calcaneus to the head of the I metatarsal bone inside and to the tuberosity of the V metatarsal bone outside divide the area into the back and the sole.
 TOPOGRAPHIC ANATOMY OF THE SOLE Skin of the pancreas Intrinsic fascia (superficial and deep leaves) Muscles: - medial group (abductor, flexor and adductor muscles of the thumb) - lateral group (muscle, abductor little finger and flexor of the little finger) - middle group (short flexor of the fingers, square muscle soles, flexor of the fingers long, peroneus longus, 4 vermiform muscles, 3 plantar interosseous muscles).
TOPOGRAPHIC ANATOMY OF THE SOLE Skin of the pancreas Intrinsic fascia (superficial and deep leaves) Muscles: - medial group (abductor, flexor and adductor muscles of the thumb) - lateral group (muscle, abductor little finger and flexor of the little finger) - middle group (short flexor of the fingers, square muscle soles, flexor of the fingers long, peroneus longus, 4 vermiform muscles, 3 plantar interosseous muscles).

 BLOOD SUPPLY Blood supply and innervation of the sole are carried out by the lateral medial and plantar arteries. Lymphatic and venous outflow is carried out in the proximal direction to the popliteal l / y, to the veins of the lower leg and the popliteal vein. Innervation is carried out by the medial and lateral plantar nerves.
BLOOD SUPPLY Blood supply and innervation of the sole are carried out by the lateral medial and plantar arteries. Lymphatic and venous outflow is carried out in the proximal direction to the popliteal l / y, to the veins of the lower leg and the popliteal vein. Innervation is carried out by the medial and lateral plantar nerves.
 LAYER-LAYER TOPOGRAPHY OF THE DARK OF THE FOOT Skin of the pancreas The intrinsic fascia (superficial and deep sheets) of the SNP is represented by the dorsal artery, companion veins, and the deep peroneal nerve. The blood supply is carried out by the dorsal artery of the foot (arcuate artery). Venous and lymphatic drainage is directed from the back of the foot from the bottom up to the popliteal l / y and vein. The skin is innervated medially by the safenus, laterally by the sural nerve, and in front by the deep and superficial peroneal nerves.
LAYER-LAYER TOPOGRAPHY OF THE DARK OF THE FOOT Skin of the pancreas The intrinsic fascia (superficial and deep sheets) of the SNP is represented by the dorsal artery, companion veins, and the deep peroneal nerve. The blood supply is carried out by the dorsal artery of the foot (arcuate artery). Venous and lymphatic drainage is directed from the back of the foot from the bottom up to the popliteal l / y and vein. The skin is innervated medially by the safenus, laterally by the sural nerve, and in front by the deep and superficial peroneal nerves.
 LAYERAL ANATOMY OF THE FINGERS Skin of the pancreas Dorsal aponeurosis Arteries, dorsum and plantar, 4 for each toe, run along the lateral sides of the toes. Venous and lymphatic drainage in the proximal direction. The medial plantar nerve innervates 3, 5 fingers from the medial side, the lateral plantar nerve - 1, 5 fingers from the lateral side. On the back of the foot, the toes innervate the branches of the peroneal nerves.
LAYERAL ANATOMY OF THE FINGERS Skin of the pancreas Dorsal aponeurosis Arteries, dorsum and plantar, 4 for each toe, run along the lateral sides of the toes. Venous and lymphatic drainage in the proximal direction. The medial plantar nerve innervates 3, 5 fingers from the medial side, the lateral plantar nerve - 1, 5 fingers from the lateral side. On the back of the foot, the toes innervate the branches of the peroneal nerves.

